Total Ankle Replacement
Just like Total Hip Replacement and Total Knee Replacement ,Total Ankle Replacement is performed to treat pain and stiffness in the ankle arising from advanced arthritis.
The most common form of arthritis affecting the ankle is osteoarthritis. Osteoarthritis is a disease of cartilage leading to loss of cartilage that eventually leads to bone grinding on bone. Similar to the loss of rubber on your car tyre that can lead to exposure of the underlying casing. This obviously is painful and can lead to swelling, stiffness and if the underlying wear is uneven then it can lead to deformity.
Ankle osteoarthritis is usually caused by trauma. This can be an old fracture or cartilage damage that has occurred from an ankle sprain. Cartilage damage can lead to progressive arthritis over time.
Instability can also lead to arthritis of the ankle – A chronically unstable ankle can lead to accumulated damage to a joint and arthritis with deformity.
Chronic malalignment either above or below the ankle joint can lead to osteoarthritis because of uneven forces that act across the joint leading to uneven cartilage wear. This can include a malunited tibial fracture or severe uncorrected flat foot deformity.
Ankle arthritis can also be caused by inflammatory arthritis such as Rheumatoid Arthritis. This is much less common than osteoarthritis.
The two main surgical treatment options are:
Ankle fusion is where surgery is done to get the tibia and talus bones to join together by preparing the joint surfaces and internally fixing with screws or plates. This obviously eliminates all movement at the ankle joint and therefore relieves pain.
The advantages of an ankle fusion are:
The disadvantages of an ankle fusion are:
The advantages of an ankle replacement are:
The disadvantages of an ankle replacement are:
An ankle replacement is done under a general anaesthetic. My Anaesthetist does an ankle block using an ultrasound machine to increase the accuracy. This provides excellent pain relief for the first 24hours after the surgery. A tourniquet is applied to the leg and the leg is prepped and draped in a standard manner.
A surgical approach to the ankle from the front is performed and this exposes the ankle joint. Using the X-ray machine in theatre a jig is applied that allows accurate cuts to be made on the bottom of the tibia and other instruments allow preparation of the talus.
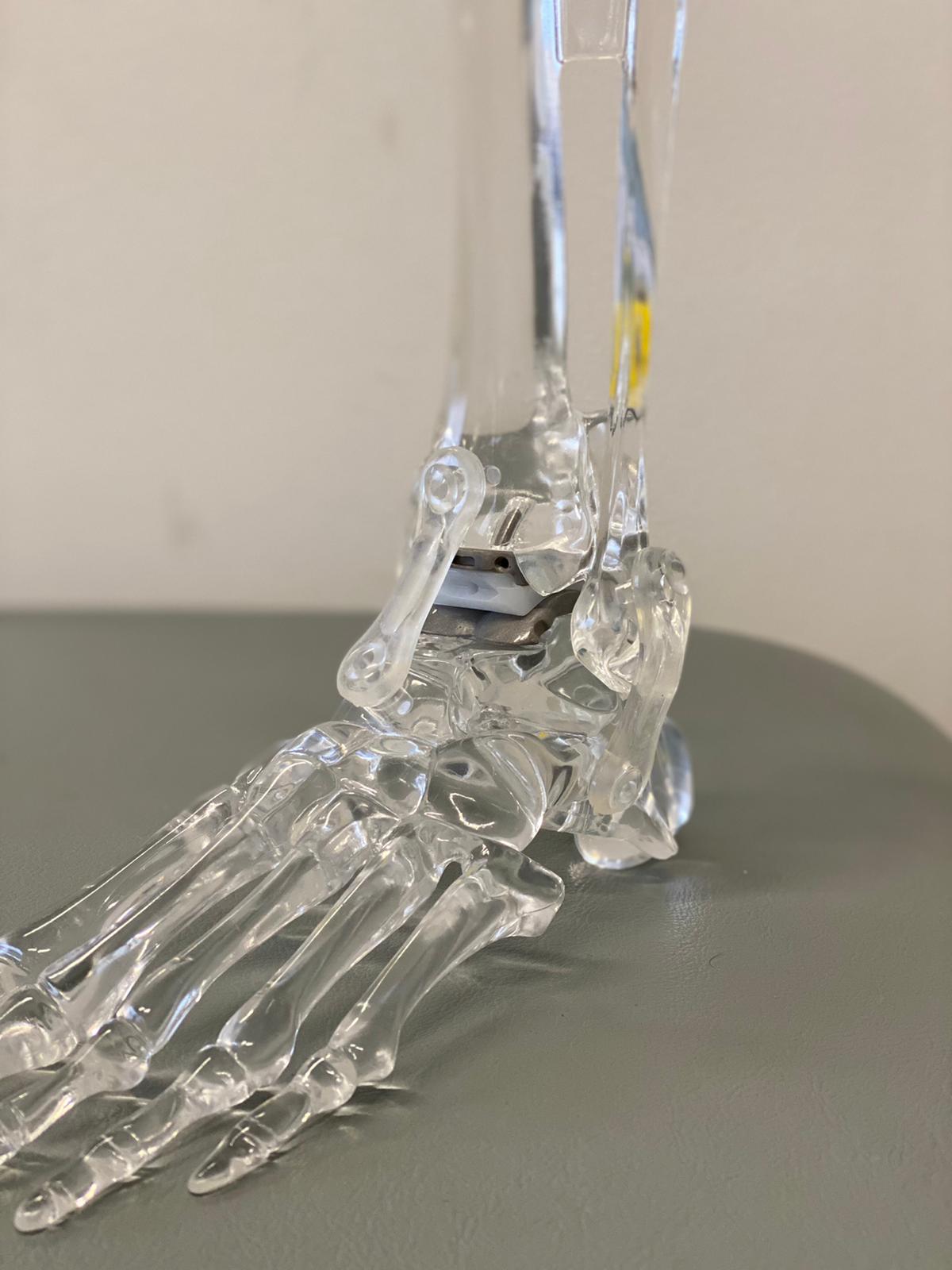
A metal plate with a roughened surface on the tibial bone side and a smooth surface on the joint side is inserted. This provides initial stability but long term stability is achieved by the bone growing onto the metal component. A similar metal cap is applied to the top of the talus and then a plastic insert ( same special plastic used in knee and hip replacements) is inserted between the metal components.
Alignment, soft tissue balancing and stability are all checked and then the wound is closed in layers and a plaster backslab(not a full cast) is then applied.
Achilles Tendon Lengthening- The achilles tendon can be very tight as part of the arthritic process and sometimes it is necessary to perform an achilles tendon lengthening at the time of insertion of the total ankle replacement.
Lateral Ligament Reconstruction- Instability can be a cause of arthritis developing in an ankle and this may need to be addressed when a total ankle replacement is inserted. Therefore a lateral ligament reconstruction is sometimes performed as part of an ankle replacement. this does not increase the recovery time.
Subtalar Joint Fusion- Subtalar joint arthritis can be present with ankle arthritis and can be a reason for incomplete pain relief following a total ankle replacement. If it is felt that there is symptomatic STJ arthritis then we sometimes perform a subtalar joint fusion either before or after the total ankle replacement depending on whether it is felt the subtalar joint or the ankle joint is the most symptomatic joint.
Correcting the alignment outside of the ankle joint is extremely important to a successful total ankle replacement and it is common to require a Heel Shift procedure in addition to the ankle replacement.
This where we perform a cut in the heel bone(calcaneus) to correct either a varus deformity where the heel curls in or a valgus deformity where it angles out.
This is often done through a keyhole procedure and fixed with a screw.
The main nerve to the foot called the Tibial Nerve passes through a fibrous tunnel on the inside of the ankle (similar to the carpal tunnel in the wrist).
It is sometimes necessary to do a prophylactic release of this tunnel (Tarsal Tunnel Release) when we are performing a heel shift.
With the heel shift the tunnel can narrow down putting pressure on the nerve and this can cause pain and/or numbness on the sole of the foot which we can avoid by performing a tarsal tunnel release before the heel osteotomy.
There are a number of other procedures that are sometimes necessary to correct associated deformity that has contributed to the development of the ankle arthritis and are necessary to achieve a well aligned and well balanced ankle joint replacement.
These can include bony and soft tissue procedures to correct a Flat Foot Deformity or a Cavus Deformity(High Arch)– These deformities are opposites but when severe they can contribute to the development of ankle arthritis.
Occasionally a patients deformity is so severe that we need to stage the ankle replacement.
That is where we do an initial procedure to correct all of the deformity but don’t do the ankle replacement and we allow this to heal.
Once it is healed then we do a second stage procedure to perform the ankle replacement. This second stage is usually straightforward because all of the deformity has been corrected.
The second stage is usually done at about three months when we are confident all of the bone and soft tissue procedures performed at that first stage have healed.
The patient’s leg is elevated and circulation observations are performed by the nursing staff overnight. A PCA(patient controlled analgesia) is provided but patients often have little or no pain because of the block. This is good because narcotic analgesics such as morphine are excellent pain relievers but some patients are very sensitive to them causing nausea and they can increase drowsiness.
Patients are usually in hospital 2-3 days. The length of time depends on how mobile the patient is and being cleared by physio. Patients are non weight bearing for six weeks. This is to allow the bone to get some early growth onto the components. To be non weight bearing they can use crutches but there are alternatives. Many patients find crutches difficult because of balance and the strain on the upper limbs. There are scooters available called the “knee walker oz” which many patients find very useful to mobilise in a safe and convenient manner. The physio can make an assessment with the patient about what is the best method to use.
The patient is also discharged home on clexane injections. This is a blood thinner which reduces the risk of DVT. These injections are maintained while the patient is non weight bearing and in a brace. That means 6 weeks. The patient and their partner/family are instructed on how to do the injections by the nursing staff prior to discharge.
The patient is then reviewed 10 days to two weeks post op so the backslab can be removed and the stitches removed. The patient is then placed in a moonboot which can be removed for showering and range of motion exercises.
We also get a doppler ultrasound to check whether there is a DVT present or not. if it is negative then the clexane is continued but if it is positive then the patient needs to go on to Warfarin or an equivalent. this is co ordinated by the patients local doctor or an outpatient service at the local hospital.
At the six week mark an xray is taken and the patient can start weight bearing as tolerated in the moonboot. The moonboot is continued for another six weeks so you are not walking without a brace for a total of 3 months after a total ankle replacement.
Some physiotherapy may be required but most of the “physio” is walking. that action strengthens the requisite muscles over time.
The patient is then followed up at the six month and 12 month postop points and then on a yearly basis after that. More frequent reviews will be performed if clinically necessary to ensure that the patient is progressing well and to monitor for any problems.
Like any surgery Total Ankle Replacement has a risk of complications. Each patient is thoroughly assessed preoperatively to identify any particular potential problems their circumstances may create and strategies are utilised to address these issues and mitigate any risks. This is part of the LRSNSW difference.
Complications can relate to the anaesthetic and these are discussed in the article on informed consent- click here
With respect to Total Ankle Replacement there is a risk of:
If a nerve is divided it can lead to permanent numbness but if it gets caught up in scar tissue this can lead to a painful condition called a neuroma.
If recognised early then it can be treated with appropriate medications and physiotherapy is a very important part of the treatment. Early review by a pain medicine specialist can help reduce the severity of the syndrome and reduce the risk of permanent problems.





Link partner: slot5000 luxury333slot.com batman138slot.com roma77 spade88 qqmobil fixbet88 hoki368 sky77 zeus138jaya.org qqnusa jackpot138 sikat138 warung138 ligaplay88 hoki99 luxury12 dewagg